

Malnutrition is not a condition confined to famine or poverty. It is happening right now, in hospitals across South Africa, to patients who arrived seeking treatment for something else entirely. It is called Disease-Related Malnutrition (DRM) and it is one of the most underdiagnosed, underreported, and under-addressed challenges in our healthcare system.
ENASA, the Enteral Nutrition Association of South Africa, is committed to changing that. This series of articles will unpack what DRM is, why it matters to clinicians and policymakers alike, and what practical steps can be taken to address it. We begin here, with the evidence.
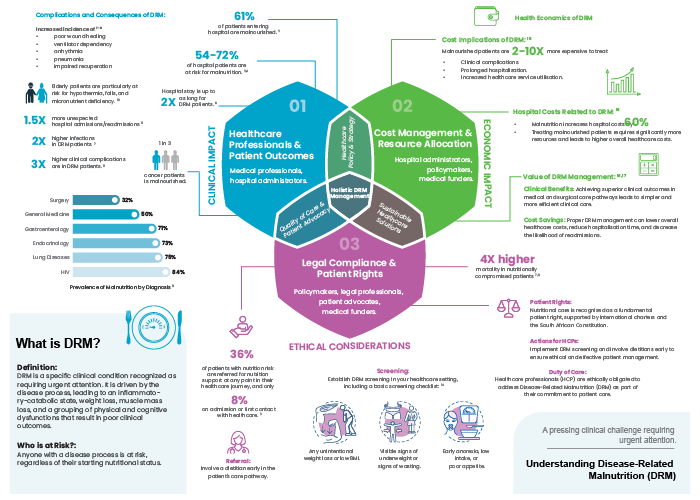
What is Disease-Related Malnutrition?
DRM is a specific clinical condition driven by the disease process itself1,2. Unlike starvation-related malnutrition, DRM is triggered by inflammatory and catabolic responses to illness or injury – leading to weight loss, muscle mass loss, impaired immune function, and a cascade of physical and cognitive dysfunctions that significantly worsen patient outcomes.
Critically, anyone with an active disease process is at risk regardless of their weight, BMI, or nutritional status on admission. A patient who appears well-nourished can be malnourished in ways that are clinically significant and prognostically important.
The scale of the problem in South Africa
South Africa carries one of the highest burdens of DRM in the world. The data is stark:
70-80% of hospitalised patients in South Africa are malnourished or at risk of malnutrition³˒⁴
61% of patients enter hospital already malnourished³
54-72% of hospital patients are at nutritional risk³˒⁴
For context: the equivalent figures in the USA sit at 35-45%, and around 45% in the EU.⁵ South Africa's burden is not just significant; it is substantially higher than comparable high-income settings, and demands a proportionate response.
The clinical consequences are severe
DRM does not simply slow recovery. It actively worsens outcomes across every clinical pathway. Malnourished patients experience:
- 2× higher rate of infections6
- 3× more clinical complications7-9
- 2× longer hospital stays⁸
- 1.5× more unexpected readmissions7
- 4× higher mortality in nutritionally compromised patients6,8
The consequences extend to specific patient populations. One in three cancer patients is malnourished. Elderly patients face heightened risk of hypothermia, falls, and micronutrient deficiency10. And across diagnosis categories, malnutrition prevalence ranges from 32% in surgery to 84% in HIV patients3.
The economic case is equally compelling
This is not only a clinical issue – it is a health economics issue. Malnourished patients cost 2-10× more to treat than well-nourished patients11. Malnutrition increases hospital costs by 60%12. Every day a malnourished patient remains hospitalised due to preventable complications is a day of unnecessary expenditure.
The inverse is equally true: proper DRM management reduces complications, shortens hospital stays, and lowers readmission rates.
Oral Nutrition Supplements (ONS) alone can reduce mortality by up to 24% and lower complication rates by 18%7,12,13.
For hospital administrators, medical funders and policymakers, the business case for addressing DRM is as strong as the clinical one.
A duty of care – and a constitutional obligation
Nutritional care is recognised internationally as a fundamental patient right. In South Africa, this is reinforced by the Constitution: Sections 27, 28 and 35 enshrine the right to food, health, and adequate care. The Global Leadership Initiative on Malnutrition (GLIM)14 provides a validated diagnostic framework that, if adopted nationally, would standardise detection and strengthen evidence-based practice.
Healthcare professionals have an ethical obligation to screen for DRM as part of routine care. That obligation begins with three simple questions on admission:
- Is there any unintentional weight loss or low BMI?
- Are there visible signs of underweight or wasting?
- Is there early anorexia, low intake, or poor appetite?
If the answer to any of these is yes, a dietitian should be involved early – not as a referral of last resort, but as an integral part of the care pathway from the outset.
What comes next?
This is the first in a series of ENASA-led articles on disease-related malnutrition in South Africa. Upcoming articles will explore the systemic and policy barriers that prevent effective DRM management, the economic burden on the healthcare system, and the ethical and constitutional imperatives for change.
Only 36% of patients identified as nutritionally at risk are referred for nutrition support at any point in their healthcare journey3. Only 8% receive that support on admission3. This is the gap ENASA is working to close – through education, advocacy and systemic change.
ENASA advocates for the recognition and treatment of disease-related malnutrition across South African healthcare settings. Visit enasa.org or contact chairperson@ena-sa.co.za | +27 66 269 1173
Note: This is sponsored content. The views and opinions expressed are those of the author(s) and do not necessarily reflect the official policy or position of MedicalBrief.
References
¹ WHO/EURO:2023-8931-48703-72392 ²Cederholm et al. 2015 ³Blaauw et al. 2019 ⁴Van Tonder et al. 2018 ⁵Norman et al. 2008 6Burgos et al. 2020 7MNI Dossier 2018 ⁸Correia et al. 2003 ⁹Demling 2009 ¹⁰Roberts et al. 11Elia et al. 2016 12Freijer et al. 2013 13Gomes et al. 2019 ¹⁴Cederholm et al. 2019