

An MPS survey of South African doctors has found that the overwhelming majority have not undertaken specific training in record keeping and want more guidance, writes Diane Baylis, clinical risk educator, Risk Prevention, Medical Protection Society.
Doctors understand the importance of good record keeping, both for themselves and for the welfare of their patients. However, an MPS survey of South African doctors has found that the overwhelming majority have not undertaken specific training and want more guidance on record keeping.
A recent survey of a sample of MPS members asking about their experience of keeping medical records received a response from 838 doctors. Respondents were from a variety of clinical backgrounds, including consultants and general practitioners in both public and private practice.
Why is medical record keeping important?
Good clinical records are a prerequisite to delivering high quality care and ensuring continuity when a number of different clinicians are contributing simultaneously to patient care. They can also be interpreted by others as marker of competence. Maintaining complete contemporaneous records also enables a doctor to provide evidence of the care given and thus is invaluable if they have a complaint or a claim of clinical negligence.
Poor record keeping can contribute to an adverse outcome such as a delayed diagnosis and could lead to a complaint, claim or a referral to the Health Professions Council of South Africa (HPCSA).
While different approaches are taken, most doctors know the importance of record keeping and feel they always keep good records themselves. Almost all survey respondents (94%) agreed that accurate record keeping is part of their professional responsibility.
Results of the survey
Despite acknowledging the importance of good record keeping, the survey has found that only 11.8% of doctors have undertaken specific training in keeping medical records and a correspondingly high proportion would like to.
The survey reports that the quality of medical record keeping in South Africa is highly variable. This inconsistency may relate to the fact that this skill is often learnt by apprenticeship rather than the application of a standard record structure. However, research shows that structured records have beneficial effects on doctor performance and patient outcomes. In the recent MPS survey, the majority (71%) of the doctors who participated said they follow a basic structure of history and then examination findings and over half (56%) said their records are handwritten, with only 9% wholly digital.
The constant drive to improve the quality and safety of medical practice, and the increasing expectations and costs of medical care, means the structure and content of the clinical record is becoming ever more important.
While the majority of doctors feel they keep good records, and half of the survey respondents reported that they have been complimented on the quality of record keeping, 8.2% have had colleague complain about their record keeping. 14% have also had a patient complaint, claim or local issue where record keeping was identified as a component. Most doctors indicated that they would like more guidance on good record keeping.
Why we don’t always keep good records?
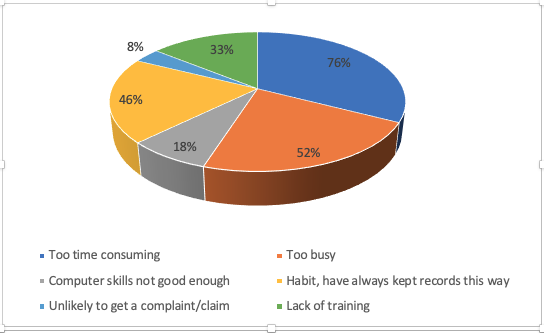
The challenges of record keeping will not be surprising to many doctors. There are many reasons why we don’t always keep good records, some relating to factors about our own attitudes and others relating to our working environment. When asked about the main barriers to keeping comprehensive records, 76% said it was too time consuming and 51% said they were too busy. Other prominent barriers include habit, insufficient computer skills and lack of training. Other issues are identified in the chart below.
MPS advice on record keeping
An adequate medical record is one that enables the doctor to reconstruct a consultation without reference to memory. A medical record is also vital in ensuring good continuity of care, so it is essential that they are as clear and complete as possible. There are four crucial components to a good medical record;
Legibility
Contemporaneous with the accurate date and time
Identifiable i.e. Printed name and signature
Up to date.
Uncertainty over the reliability of a medical record can be caused by poor or illegible handwriting, alterations or late additions that cannot be sufficiently explained. It is perhaps only human for a doctor dealing with an impending negligence claim, when realising that details are not fully documented in the medical record, to make a late alteration/addition. If you do need to make an alteration/addition, make sure you are completely overt and enter the date, your name and reason for the addition, so there can be no unjustified suspicion.
Accurate medical record keeping is also part of the ethical and professional guidelines of the HPCSA. This states that as doctors you have a professional obligation to keep accurate and good quality records1:
• Records should be complete, but concise.
• Records should be consistent.
• Self-serving or disapproving comments should be avoided in patient records. Unsolicited comments should be avoided.
• A standardised format should be used (e.g. notes should contain in order the history, physical findings, investigations, diagnosis, treatment and outcome.).
• If the record needs alteration in the interests of patient care, a line in ink should be put through the original entry so that it remains legible; the alterations should be signed in full and dated; and, when possible, a new note should refer to the correction without altering the initial entry.
• Copies of records should only be released after receiving proper authorisation.
• Billing records should be kept separate from patient care records.
• Attached documents such as diagrams, laboratory results, photographs, charts, etc. should always be labelled. Sheets of paper should not be identified simply by being bound or stapled together – each individual sheet should be labelled.
You should consider documenting the following:
• Others present, e.g. a chaperone, name of the chaperone used, or if one was declined; other family members present
• Discussion with patient/relatives such as shared decision making, consent
• Important questions answered and information that was given, e.g. treatment options, risks and benefits, prognosis along with any self-management advice or leaflet given
• History including negative and positive findings, red flags, discriminators
• Examination findings including objective measurements
• Diagnosis
• Investigations and treatment plan including referrals, medication
• Follow up and safety net; progress if a review.
Summary
Good medical records, whether electronic or handwritten, are a vital component of providing good quality clinical care and are essential for the continuity of care of your patients.
For doctors, good medical records are vital as they provide a window on the clinical judgment being exercised at the time. Adequate medical records that enable you or somebody else to reconstruct the essential parts of each patient contact should also contain the information required should they be required for legal purposes if, for example, the patient pursues a clinical negligence claim.
MPS will be providing further training on this subject later this year.
References
1
[link url="https://www.hpcsa.co.za/?contentId=0&menuSubId=18&actionName=Core%20Operations"]HPCSA, Ethical guidelines for good practice in the health care professions, Booklet 9: Guidelines on Patient Records (Sept 2016):[/link]