

WHO recognises priority of Disease-related Malnutrition
In 2023, the WHO1 published a call to action on disease-related malnutrition (DRM) as an under-recognised and inconsistently managed healthcare issue. Since DRM is driven by the physiology of acute and chronic disease conditions, it deserves integration into clinical health services and management protocols. While the global prevalence of DRM is at least 30%-45%, South Africa is unduly burdened with at least double that prevalence2. Despite this, South African hospitals may only actively identify a third of these patients and actively intervene in 15% of those at risk3.
What’s at stake – counting the cost
This low responsiveness to the significant healthcare risk of DRM is not without consequences. In a healthcare environment increasingly oriented to outcome quality metrics, clinical and funder stakeholders should pay urgent attention. The link between DRM and worse clinical outcomes is extremely well described and robust, and generally proportional to degree of nutritional compromise. Patients with DRM have:
● 2-3x more clinical complications including infections, poor wound healing, surgical site dehiscence, ventilator dependency, arrhythmia, pneumonia and impaired recovery4-7
● 4-10x lower survival4,5
● 1-2x longer hospital stays and more hospital admissions4,5
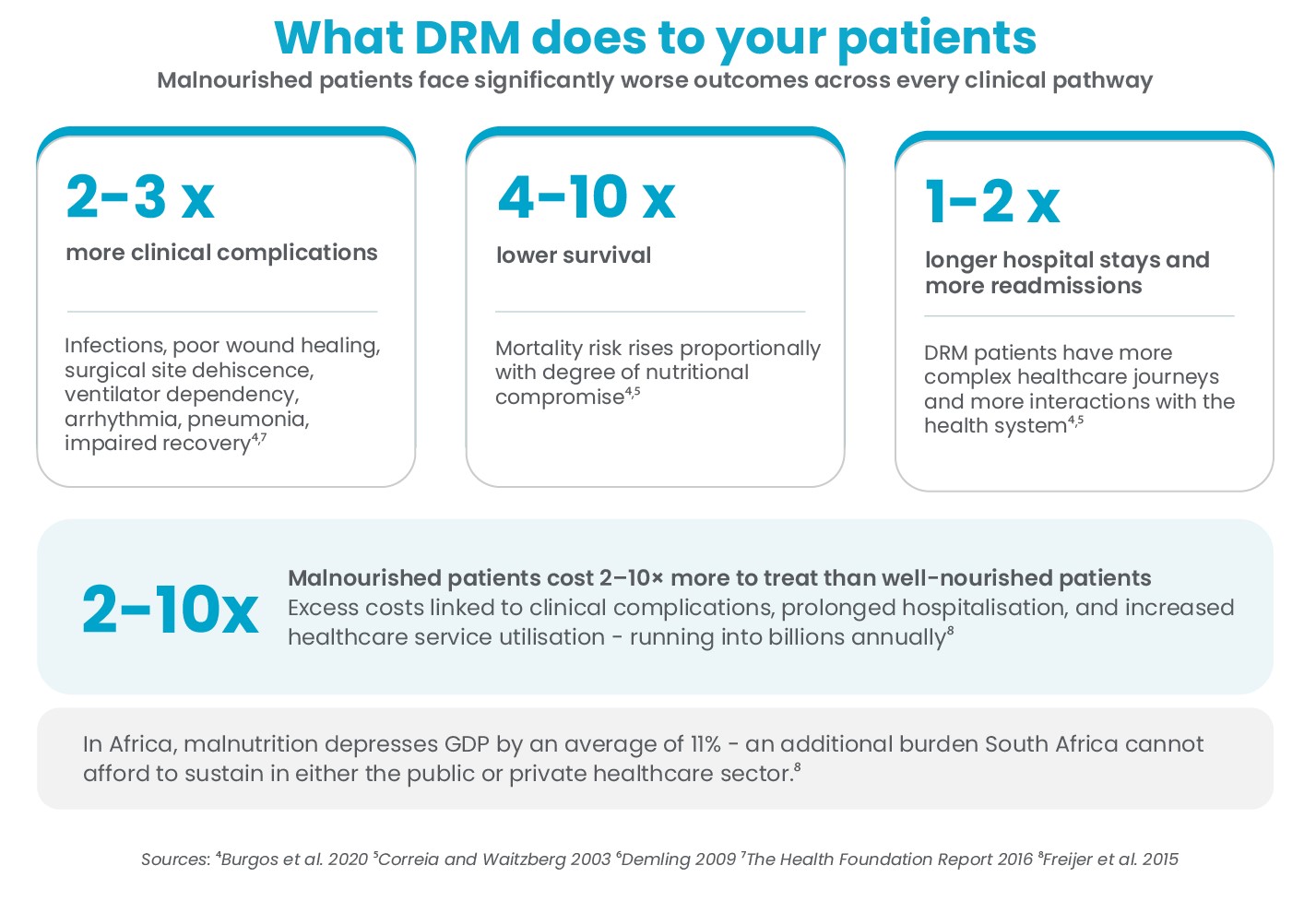
Therefore, malnourished patients have a more clinically complicated disease course and more complex healthcare journeys. Since this translates into more interactions with the health system and higher use of healthcare resources, it is obvious that DRM makes patients more expensive to treat.
Resource-constrained healthcare settings such as South Africa are obligated to take cost into consideration. Evidence indicates that the excess cost of healthcare related to morbidity management in DRM is at least twice (but may be up to tenfold) the base per patient health expenditure, running into billions of euros or dollars annually8.
In Africa, malnutrition depresses GDP by 11% on average. Clearly, this is an additional health cost burden that a country like South Africa cannot afford to sustain in either the public or the private healthcare sector.
Value of nutrition support
Fortunately, there is a solution to both the clinical and health economics implications of DRM. There is no argument that medical nutrition therapy, including skilled dietetic management, therapeutic diets and oral nutrition supplements as well as artificial nutrition support in the form of enteral and parenteral nutrition, is highly effective in producing better clinical outcomes and reducing complications for multiple patient types in both health facilities and in out-patient care9. This approach is supported by both the WHO and the international clinical nutrition professional community and demonstrated by an abundance of scientific literature.
Added value
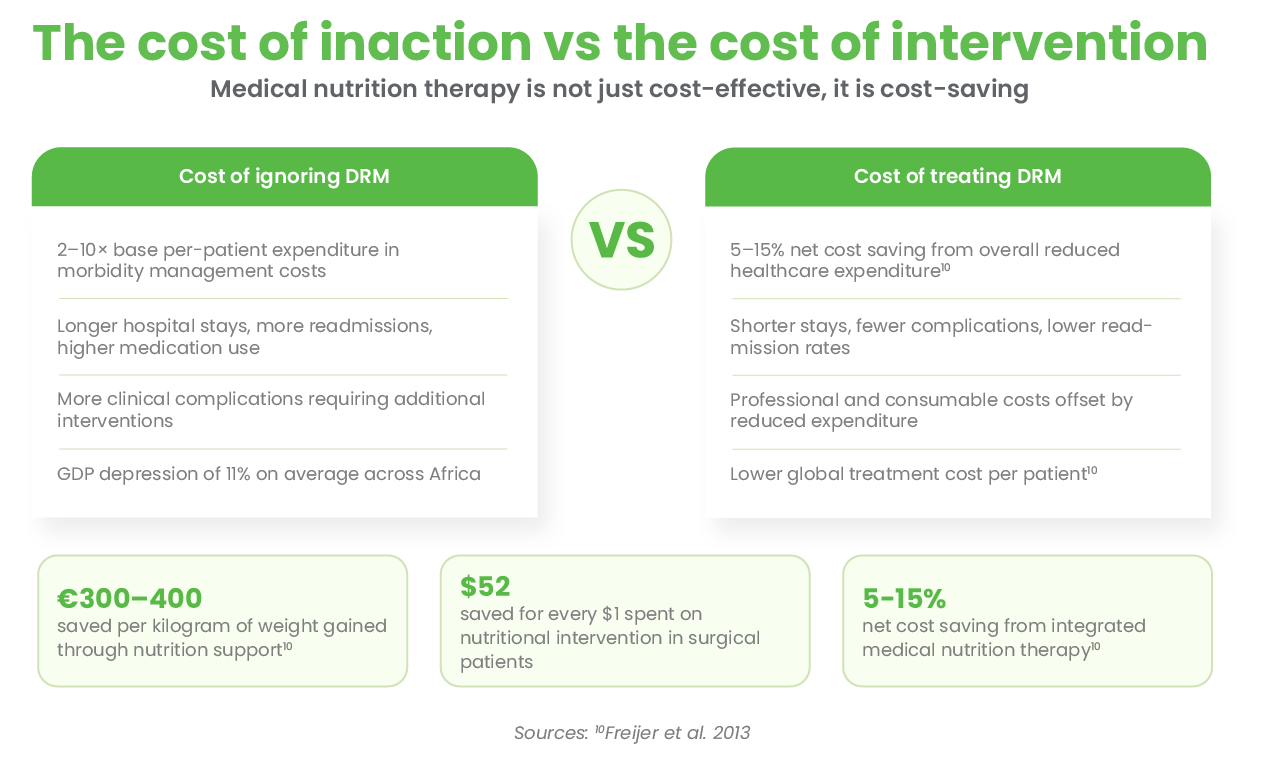
The value of clinical nutrition support in fact goes beyond clinically measurable improvements in outcome, including mortality. Pro-actively investing in intentional therapeutic nutritional support of patients with DRM reduces costs through shorter stays, fewer complications, lower medication use and improved survival.
Indeed, multiple health economic analyses have shown medical nutrition therapy to be not only cost-effective, but cost-saving10. The combined professional and consumable costs of delivery medical nutrition to DRM patients is offset by the 5%-15% net cost saving from overall reduced healthcare expenditure. This means a lower global treatment cost per patient10 – an issue that should be of intense interest to public and private healthcare reimbursement structures under ongoing financial pressure in the current health climate.
Measurable specifics on cost savings
Cost containment associated with nutrition support has been calculated to be:
● €300-400 saved per kilogram of weight gained10
● $52 saved for every $1 spent on nutritional intervention in surgical patients
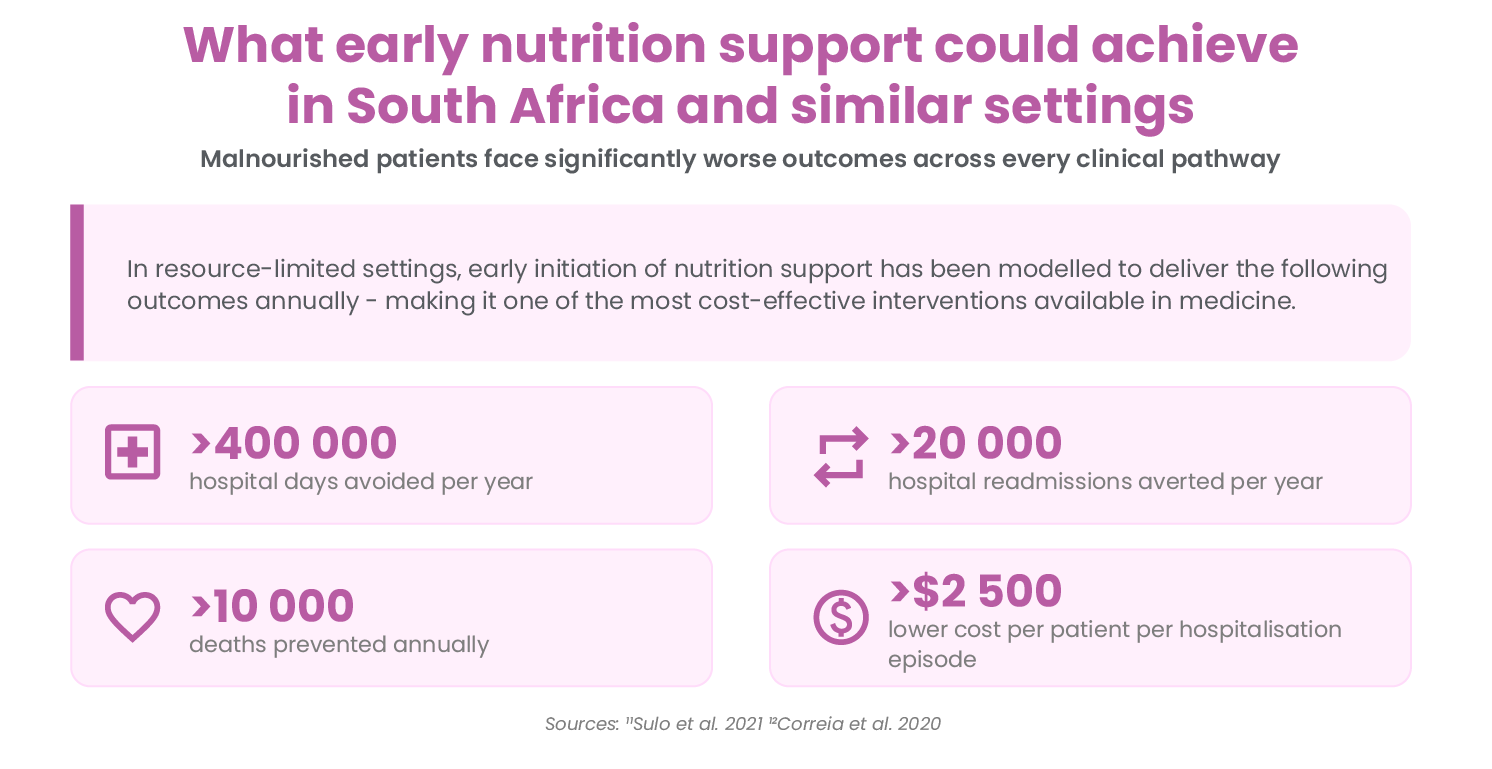
In low- and middle-income countries (LMIC)11,12, early use of nutrition support has been modelled to result in:
● > 400 000 avoided hospital days per year,
● > 20 000 averted hospital readmissions per year
● >10 000 annual deaths prevented
● >$2 500 lower cost per patient per hospitalisation episode
Priority patients
While nutrition support has a substantial impact on health costs, a system which full supports integrated medical nutrition therapy for every patient will not be built or financed overnight. It is rational to recognise that some sub-groups of patients should be prioritised for their higher inherent risk. The risk of DRM is particularly increased by acute and chronic inflammatory states, frailty and ageing. Therefore, patients with any form of cancer, chronic kidney/liver/lung diseases, infectious diseases such as HIV and TB, those with gastrointestinal diseases and the elderly are groups that should be considered especially vulnerable deserving of special monitoring.
Next steps
In the next article in this series the case for improved policy support and integrated health protocol response will be outlined within the context of a human rights-based healthcare framework and the resource-limited setting of South Africa.
ENASA – the Enteral Nutrition Association of South Africa – advocates for the recognition and treatment of disease-related malnutrition across South African healthcare settings.
Visit enasa.org or contact chairperson@ena-sa.co.za | +27 66 269 1173
References
¹WHO/EURO:2023-8931-48703-7239 2Blaauw et al. 2019 3Van Tonder et al. 2023 4Burgos et al 2020 5Correia and Waitzberg 2003 6Demling 2009 7The Health Foundation Report 2016 8Freijer et al 2015 9MNI Dossier 2018 10Freijer et al 2013 11Sulo et al 2021 12Correia et al 2020